By ProHobby™ | Ecological Systems Authority
Every disease treatment article on this site — ich, fin rot, velvet, dropsy, Columnaris, popeye, gill flukes, hole in the head disease, anchor worm, Camallanus worms, and Malawi bloat — references treating in a hospital tank rather than the main display. Most hobbyists skip this step because they do not have a hospital tank set up when disease appears. They treat in the main tank instead, damage the biological filtration, cause an ammonia spike, and lose fish not to the original disease but to secondary ammonia poisoning during treatment. Or they avoid treatment entirely because setting up a separate tank mid-crisis feels overwhelming.
This article removes both obstacles. A hospital tank can be set up in 20 minutes from equipment you likely already have, or can be maintained in a state of permanent readiness with minimal effort. Understanding why it exists — and specifically understanding the central conflict between medication and biological filtration that makes it necessary — makes every treatment decision clearer.
Table of Contents
- Hospital Tank vs Quarantine Tank — The Distinction Matters
- Why Treating in the Main Tank Is the Wrong Default
- The Core Problem: Medication vs Biological Filtration
- What a Hospital Tank Actually Needs
- The Pre-Prepared Hospital Tank — Permanent Readiness
- The Emergency Setup — When Disease Appears Without Warning
- Managing Water Quality Without a Cycled Filter
- Medication and Water Changes — The Dosing Protocol
- Stress Minimisation — The Environment Matters
- Species-Specific Hospital Tank Considerations
- The Return Protocol — Moving Fish Back Safely
- Between Uses — Decontamination and Storage
- Frequently Asked Questions
1. Hospital Tank vs Quarantine Tank — The Distinction Matters
These two tank types are frequently used interchangeably in aquarium guides. They serve related but distinct purposes and are set up and managed differently.
A quarantine tank receives new, apparently healthy fish for a 4-week observation period before main tank introduction. Its purpose is disease prevention — observing whether subclinical disease establishes during the post-transport immune vulnerability window. It ideally has an established biological cycle, no medication, and stable, low-stress conditions. The complete quarantine protocol for new fish is in Quarantine and Biosecurity in Aquariums.
A hospital tank receives sick fish for active treatment. Its purpose is disease resolution — providing an isolated environment where medication can be administered at precise concentrations without affecting the main display, where the sick fish can be closely monitored, and where biological filtration disruption from medication does not crash the main tank’s nitrogen cycle.
The same physical tank can serve both purposes — many hobbyists maintain a single spare tank that functions as quarantine for new arrivals and hospital for sick fish, with appropriate cleaning and setup changes between uses. But the management approach is different for each use case.
The diagnostic framework for determining whether a sick fish needs a hospital tank (true pathogenic disease requiring medication) or whether environmental correction in the main tank is the correct response is in Quarantine vs Medication in Aquariums. That framework should be applied before any treatment decision.
2. Why Treating in the Main Tank Is the Wrong Default
The instinct to treat disease in the main display tank is understandable — the fish are already there, the water is cycled, and setting up a separate tank requires effort. In almost every case, it is the inferior approach.
Biological filtration destruction. Most aquarium medications — antibiotics, copper, malachite green, formalin, metronidazole — damage or kill nitrifying bacteria in the filter and substrate biofilm. A standard antibiotic course in the main tank can effectively un-cycle a tank that took months to mature. Ammonia rises within 24–48 hours of beginning treatment. The fish that was being treated for fin rot now has fin rot and ammonia poisoning simultaneously. The complete biofilm science is in Biofilms — The Invisible Engine of Every Aquarium.
Dosing inaccuracy. Correct medication dosing requires knowing the actual water volume being treated. Main display tanks contain substrate, hardscape, and water at non-labelled levels. The Aquarium Volume Calculator calculates actual volume accurately — but a 200-litre display tank with 30kg of substrate and substantial hardscape may hold only 140 litres of water. Underdosing produces treatment resistance; overdosing produces toxicity. A 30-litre bare hospital tank has essentially its stated volume minus a small PVC hide.
Carbon and substrate absorption. Activated carbon adsorbs most medications before they reach therapeutic concentration. Substrate and live rock bind copper and some antibiotics, further reducing bioavailable concentration. A hospital tank with bare bottom and no chemical filtration delivers full medication concentration to the water column.
Harm to healthy inhabitants. Copper kills invertebrates. Salt at therapeutic concentrations damages freshwater plants. Many antibiotics affect biological filtration of every tank organism, not just the target pathogen. Treating in the display tank exposes all inhabitants to a treatment designed for one.
Difficulty monitoring the patient. In a display tank with plants, hardscape, and multiple fish, monitoring one sick individual’s behaviour, appetite, waste, and progression is difficult. In a bare, simple hospital tank, every detail of the patient’s condition is visible.
3. The Core Problem: Medication vs Biological Filtration
This is the central challenge of hospital tank management and the reason it requires more active management than a standard aquarium.
Biological filtration — the Nitrosomonas and Nitrospira bacteria that convert toxic ammonia to nitrate — lives in biofilm communities on filter media, substrate surfaces, and tank walls. These bacteria are sensitive to the same chemical agents that kill pathogens. Most aquarium medications are broadly antimicrobial by nature.
When medication is added to a biologically active tank, nitrifying bacteria are damaged or killed alongside the target pathogen. The ammonia processing capacity of the filter falls. Ammonia accumulates from fish waste. The sick fish — already physiologically compromised — is now also experiencing ammonia toxicity.
The resolution: The hospital tank is managed not as a stable biological system but as a semi-managed chemical system. Either biological filtration is protected from medication (using a removable seeded sponge that is taken out before treatment begins), or biological filtration is accepted as absent and ammonia is managed through frequent water changes and ammonia detoxifier.
Both approaches work. The choice between them depends on whether you have a pre-seeded sponge available, the severity of illness, and the treatment duration required.
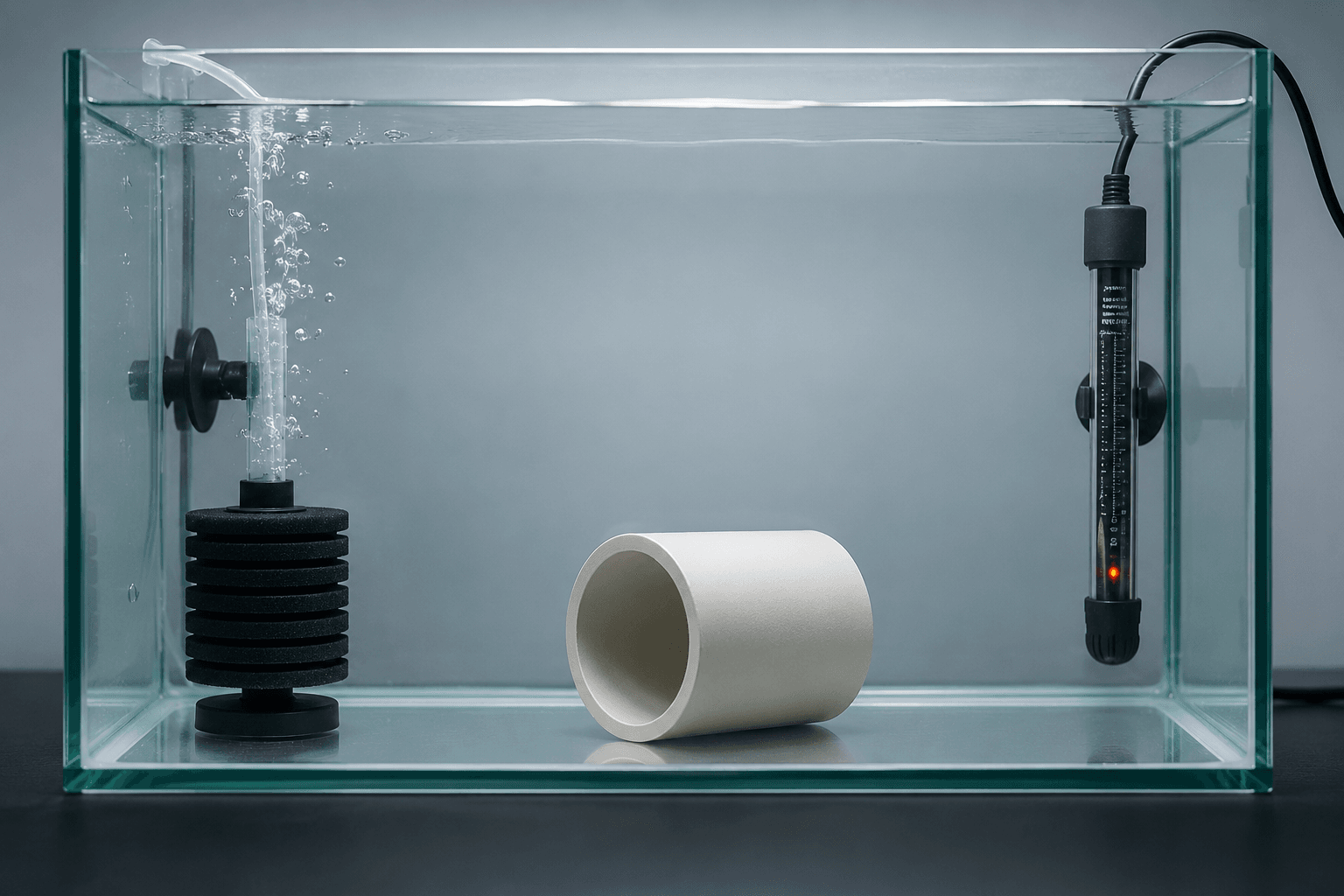
4. What a Hospital Tank Actually Needs
The hospital tank is intentionally minimal. Every addition that makes a display tank attractive creates management complications in a treatment context.
Tank size: 20–40 litres for most community fish. Large enough for normal swimming behaviour. Small enough that medication cost is manageable and that the ammonia load from one or a few fish can be controlled through water changes alone if necessary. For large fish (cichlids over 15cm, large goldfish), scale up to 60–80 litres.
Filter: A sponge filter powered by an air pump. Sponge filters are the correct choice for hospital tanks for three reasons: they can be removed before copper or antibiotic treatment begins (protecting the seeded biological media from medication), they are easily decontaminated between uses, and they cannot injure already-compromised fish through impeller suction or strong flow.
Heater: Adjustable. Many treatments require specific temperature ranges — ich treatment at 28–30°C, velvet treatment at 28–30°C, standard bacterial treatment at species-appropriate temperature.
Lid: Essential. Sick fish jump. Surface gasping brings fish close to the waterline. A cover prevents losses.
No substrate: Bare glass bottom. This is correct, not a compromise. Bare bottom allows visual inspection of droppings (colour, consistency, presence) which provides diagnostic information. Waste does not accumulate in substrate and decompose, contributing to ammonia. Medication is not adsorbed by substrate. Cleaning between uses is complete with a single rinse rather than requiring substrate removal.
Minimal décor: One piece of PVC pipe or a half-submerged terracotta pot provides cover for stressed fish without creating surface area that absorbs medication. No plants — most medications damage aquatic plants, and plants create oxygen-consumption complexity during treatment.
Thermometer: Visible, accurate. Temperature monitoring is more important during treatment than in normal aquarium management — treatment efficacy and fish physiological stress both depend on stable, correct temperature.
5. The Pre-Prepared Hospital Tank — Permanent Readiness
The ideal hospital tank is ready to receive a sick fish within 15 minutes at any time. This is achieved by maintaining it in a permanent state of preparedness between uses.
The seeded sponge approach:
Run a spare sponge filter inside an established main display tank continuously. The sponge colonises with the main tank’s biological community and maintains full biological capacity through continuous exposure to the display tank’s water and waste. When disease appears:
- Remove the seeded sponge from the display tank
- Install it in the hospital tank with fresh, dechlorinated, temperature-matched water
- Add the sick fish
The hospital tank has instant biological filtration from the seeded sponge. Ammonia is processed immediately. This is the most reliable approach for maintaining good water quality during treatment — with one critical caveat. When medication begins:
Remove the seeded sponge before adding any medication. Place it back in the display tank (where it will maintain its community) or in a bucket of aerated, dechlorinated tank water. After the treatment course is complete, return it to the hospital tank to support recovery and post-treatment monitoring.
The sponge sacrificed during medication is a small, sponge-only filter. Not the display tank’s primary filtration. This is the correct trade.
Dry storage between uses: If maintaining a running tank between uses is not practical, store a clean spare sponge filter in a Ziplock bag in a cool dry location. Before use, seed it by running it in the display tank for minimum 48 hours (longer is better), or use the seeded-sponge-from-display approach above.
6. The Emergency Setup — When Disease Appears Without Warning
For hobbyists who do not have a pre-prepared hospital tank and discover disease today, this is the 20-minute setup protocol:
What you need:
- A bucket, tub, or spare tank of any size appropriate for the fish (20+ litres)
- Air pump and airstone (or sponge filter if available)
- Heater if needed for temperature adjustment
- Dechlorinator that neutralises chloramine, not just chlorine
- Seachem Prime or equivalent ammonia detoxifier
- A lid or cover
Step 1: Fill with tap water. Add full-spectrum dechlorinator at the dose for the volume. If using a bucket or tub, a lid made of a cutting board or light cover works. Test temperature and adjust heater accordingly.
Step 2: Add an airstone or sponge filter for oxygenation and surface agitation. This setup has no biological filtration — ammonia management is entirely through water changes and ammonia detoxifier.
Step 3: Dose Seachem Prime (or equivalent) at the ammonia-detoxification rate for the total volume. This provides 24–48 hours of ammonia detoxification while the biological filtration is absent.
Step 4: Transfer the sick fish. Float the bag or container for 15 minutes before releasing.
Step 5: Test ammonia every 6–12 hours. Re-dose Prime when ammonia tests positive. Perform 25–30% water changes daily to export ammonia. After each water change, re-dose medication to compensate for the dilution.
This emergency setup is not ideal — the daily management burden is higher than a seeded-sponge approach, and frequent water changes with medication re-dosing is more demanding. But it is infinitely better than treating in the main display, and it keeps the sick fish isolated and manageable while the disease is addressed.
7. Managing Water Quality Without a Cycled Filter
Whether using an emergency setup or treating with medication that has killed the seeded sponge, the principle is the same: replace biological processing with chemical management (ammonia detoxifier) and mechanical export (water changes).
Daily ammonia testing is non-negotiable. A sick fish in an uncycled hospital tank can produce a toxic ammonia reading within 12–24 hours. Test every morning. Any positive reading above 0.25 ppm triggers an immediate partial water change.
Use the Aquarium Volume Calculator to confirm the exact volume of the hospital tank — dosing Seachem Prime or any ammonia detoxifier to a volume 20% different from actual is the difference between adequate and inadequate detoxification.
The ammonia-detoxifier protocol: Dose Seachem Prime (or equivalent) at the manufacturer’s detoxification dose (typically 5mL per 40L) every 24–48 hours throughout treatment. Prime temporarily converts ammonia to a less toxic bound form that the nitrifying bacteria process when they recover. In an uncycled tank with no nitrifying bacteria, this provides a 24–48 hour ammonia safety window — not a permanent solution, but sufficient when paired with daily partial water changes.
Test both ammonia and nitrite daily. In a tank cycling from scratch, nitrite appears after ammonia. Any positive nitrite in a hospital tank during medication indicates partial biological establishment and requires the same management as ammonia — water change and detoxifier.
8. Medication and Water Changes — The Dosing Protocol
This is where most hospital tank management fails.
Each water change removes medication proportional to the change volume. A 30% water change removes 30% of the medication. If this is not replaced, the treatment concentration falls below therapeutic levels, potentially allowing pathogen adaptation while continuing to stress the fish and damage biological filtration without achieving treatment.
The protocol:
- Before each water change, note the current medication dose and the hospital tank volume
- Perform the water change
- After the water change, re-dose medication at the percentage of the tank volume changed
Example: Hospital tank 30 litres. Ich treatment requires 2g salt per litre = 60g total. Daily 30% water change = 9 litres changed. Add 9L of new dechlorinated water. Re-dose 30% of the original salt = 18g dissolved in the new water before adding.
This applies to every medication: salt, copper, commercial ich treatments, antibiotics. The volume calculation determines replacement dose. Use the Water Change Calculator alongside the Aquarium Volume Calculator for consistent calculations throughout treatment.
The water change frequency and the medication protocol for each disease are covered in the disease-specific guides: Ich, Fin Rot, Velvet, Dropsy, Columnaris, Popeye, Gill Flukes, Hole in the Head, Anchor Worm, Camallanus Worms, and Malawi Bloat. The complete water change protocol is in How to Do a Water Change.
9. Stress Minimisation — The Environment Matters
A sick fish in a bare glass box under full lighting is a stressed fish. Stress elevates cortisol, suppresses immunity, and directly counteracts the recovery the hospital tank is designed to support. The physiology of how stress hormones suppress immune function — and why a stressful treatment environment extends recovery time — is in The Science of Fish Stress. The treatment environment should reduce rather than compound physiological stress.
Cover three sides. Tape dark paper, card, or black plastic to three walls of the hospital tank. This reduces the visual stimulus of movement outside the tank and eliminates the reflections that stress fish in bare glass tanks.
Provide one hiding spot. A piece of PVC pipe or a half terracotta pot costs nothing and dramatically reduces stress in hiding-prone species. Stressed fish spend energy on stress responses rather than recovery. A fish that can retreat to cover spends less time in acute stress states.
Maintain appropriate photoperiod. Exception: velvet treatment requires complete darkness — see Velvet Disease — Complete Treatment Guide. For all other conditions, a normal 8–10 hour photoperiod with subdued lighting is appropriate.
Maintain temperature stability. Temperature fluctuations are themselves an immune stressor. A heater with a reliable thermostat and a thermometer checked twice daily ensure the treatment temperature is held consistently. Temperature stability during ich treatment at 28–30°C is particularly important — falling back to 25°C during treatment restarts the slower lifecycle cycle that extends required treatment duration. Aquarium Water Temperature in Indian Summer covers temperature management during power cuts, which are a specific risk during Indian summer treatment periods.
Maintain dissolved oxygen. Many medications reduce dissolved oxygen. Sick fish with gill damage have reduced oxygen extraction capacity. Maximum surface agitation throughout treatment is always correct. Battery backup for the air pump prevents oxygen crisis during power cuts. The complete dissolved oxygen guide for crisis situations is Aquarium Dissolved Oxygen — Complete Guide.
10. Species-Specific Hospital Tank Considerations
Scaleless fish (loaches, many catfish) Scaleless species are extremely sensitive to most commercial medications, particularly malachite green and formalin-based products. Use half-dose and monitor closely. Salt at standard therapeutic doses (1–3g/L) is also poorly tolerated. For scaleless fish, heat treatment with maximum aeration is the safest first approach, with careful dose-reduction medication only if heat alone is insufficient.
Invertebrates (shrimp, snails, crabs) Never medicate in a tank containing invertebrates. Copper at therapeutic doses is lethal to all invertebrates. Salt at therapeutic doses is harmful to shrimp and freshwater snails. Move all invertebrates to a separate, medication-free container before any treatment. After treatment, remove medication completely through water changes before returning invertebrates.
Labyrinth fish (bettas, gouramis) Labyrinth fish breathe atmospheric air at the water surface. In a heavily medicated, low-oxygen hospital tank, ensure the surface is accessible and not obstructed. These species are generally medication-tolerant but sensitive to copper — use copper-containing products at the lower end of the recommended range and monitor closely.
Marine fish Marine hospital tanks require a protein skimmer in addition to the sponge filter — marine fish produce significantly more dissolved organic waste than freshwater fish. Salinity must be maintained at the same level as the display tank throughout treatment. Copper treatment requires a calibrated copper test kit to maintain the narrow therapeutic range. Never return copper-treated water or equipment to a reef display system.
Large cichlids and messy fish Goldfish, large cichlids, and other high-bioload species produce waste rapidly. A 30-litre hospital tank servicing a 20cm cichlid will require multiple daily partial water changes to maintain safe ammonia levels without biological filtration. Scale up the hospital tank size for large fish, or plan for three or more daily water changes of 20–30%.
11. The Return Protocol — Moving Fish Back to the Main Tank
The hospital stay is over when the disease has been treated, medication has been completed, the fish has recovered to normal behaviour and appetite, and a period of 3–5 days post-treatment has confirmed no recurrence.
Before returning fish:
Ensure the treatment course was complete — not simply that the fish looks recovered. Ich treatment must continue for the full lifecycle period after the last spot disappears. How to Clean an Aquarium Filter Without Killing Bacteria — or rather, how not to clean it — is relevant here: do not clean the hospital tank filter before assessing whether the fish needs the hospital longer.
Remove all medication from the hospital tank water through water changes before the return. For copper, this requires multiple complete water exchanges. For salt, gradual dilution through water changes over several days. For most commercial medications, 2–3 full water changes restore the water to essentially unmedicated condition.
Acclimate to main tank chemistry. The hospital tank water may have drifted in pH, KH, or temperature from the main display during the treatment period. Gradual acclimation — adding small amounts of main tank water to the hospital tank over 1–2 hours before transfer — prevents chemistry shock. Aquarium pH — Complete Diagnosis and Fix Guide covers the pH shock mechanism.
Return during a stable period. Do not return fish on the same day as a large water change, filter cleaning, or any other maintenance event that may have temporarily stressed the main tank’s biological system. Allow 48 hours of stable conditions before introduction.
Monitor the returning fish. A fish that spent time in a hospital tank is re-entering the social environment of the display tank. Existing fish may show temporary aggression toward the returning individual. Monitor for the first 48 hours.
12. Between Uses — Decontamination and Storage
A hospital tank that is not properly decontaminated between uses can transfer pathogen residue to the next patient and re-introduce disease to the display tank if the sponge filter is re-used without treatment.
Full decontamination protocol after use:
Empty the tank completely. Remove all equipment (heater, airstone, PVC hide).
Prepare a dilute bleach solution: 10ml of unscented household bleach per litre of water.
Fill the tank to 50% with the bleach solution. Submerge all equipment (heater, airstone tubing, PVC pipe, thermometer). Leave for 30 minutes.
Drain completely. Rinse minimum five times with tap water. The tank and all equipment must have no residual chlorine smell.
For the sponge filter: the sponge used during a medication course is best discarded rather than cleaned and reused. It carries medication residue in the sponge matrix that thorough rinsing does not remove. Replace with a new sponge for the next use.
Allow all equipment to dry completely before storage. Most aquatic pathogens cannot survive complete desiccation.
Storage: Store dry in a clean container. Keep the air pump, tubing, airstone, heater, and thermometer together as a “hospital kit” so the setup requires minimal time when needed.
Frequently Asked Questions
Does a hospital tank need to be cycled? Ideally yes — a seeded sponge filter from the display tank provides instant biological capacity. In practice, many hospital tanks are set up without an established cycle when disease appears unexpectedly. An uncycled hospital tank is managed through daily ammonia testing, ammonia detoxifier, and frequent water changes. This is more demanding but entirely workable and still far better than treating in the main display.
What size hospital tank do I need? For most community fish under 8cm: 20 litres minimum. For medium fish (8–15cm): 30–40 litres. For large fish (15cm+): 60–80 litres. The tank must be large enough for normal swimming without crowding but small enough that medication costs are manageable and ammonia can be controlled through partial water changes.
Can I use a bucket as a hospital tank? Yes for short-term emergencies. A clean food-grade bucket with an air pump and heater can function as a hospital tank for small fish for a treatment period. Limitations: no lid (fish can jump out), restricted swimming space, no easy observation of the fish from the side. A small spare aquarium is significantly better but a bucket is better than nothing and better than treating in the main tank.
Why can’t I just treat in my main tank? Several reasons make main tank treatment the inferior option in most cases: medication kills biological filtration, causing ammonia accumulation; substrate and activated carbon absorb medication, making dosing inaccurate; invertebrates and sensitive species are exposed to medication intended for another fish; the treated fish is harder to monitor in a complex environment; and biological filtration recovery after the treatment course can take weeks. See Section 2 for the complete argument.
How do I maintain the hospital tank between disease outbreaks? The most practical approach: run a spare sponge filter inside your main display tank continuously. When disease appears, the sponge is immediately available with an established biological community. The secondary approach: store a clean spare sponge and dry equipment, seeding the sponge in the display tank for 48–72 hours when a hospital tank is needed.
How long does a fish need to stay in the hospital tank? Until the complete treatment course is finished, the medication has been removed, and the fish shows 3–5 days of normal behaviour and appetite post-treatment. For ich: minimum 10–14 days at treatment temperature after the last visible spot. For velvet: 10–14 days of continuous treatment. For fin rot: until the fin margin has stabilised and shows early regeneration. Do not return fish to the main tank as soon as they look recovered — this often precedes a recurrence by a few days.
My hospital tank has no filter — is that okay during treatment? For short-term emergency treatment (3–5 days) in a lightly stocked hospital tank with daily water changes and ammonia detoxifier: manageable. For longer treatments (10–14 days for ich or velvet): challenging but possible with multiple daily water changes. The seeded sponge approach is strongly preferred for any treatment longer than 5 days. Without any filtration or aeration, even short-term holding creates unacceptable ammonia risk for a physiologically compromised fish.

